Table of Contents
Artificial Rupture of Membranes: What You Need to Know
Artificial rupture of membranes (AROM), also known as amniotomy or “breaking the water“, is a procedure in which the amniotic sac that surrounds the baby in the womb is intentionally ruptured by a healthcare provider.
This procedure may be done for various reasons during labor, such as to induce or speed up contractions, to monitor the baby’s heart rate more closely, or to check the amniotic fluid for signs of infection or fetal distress.
How is Artificial Rupture of Membranes (AROM) performed?
AROM is usually performed when the cervix is dilated at least 2 cm and the baby’s head is low in the pelvis. The healthcare provider will insert a gloved finger or a sterile instrument (such as an amnihook or amnicot) through the cervix and make a small tear in the membranes.
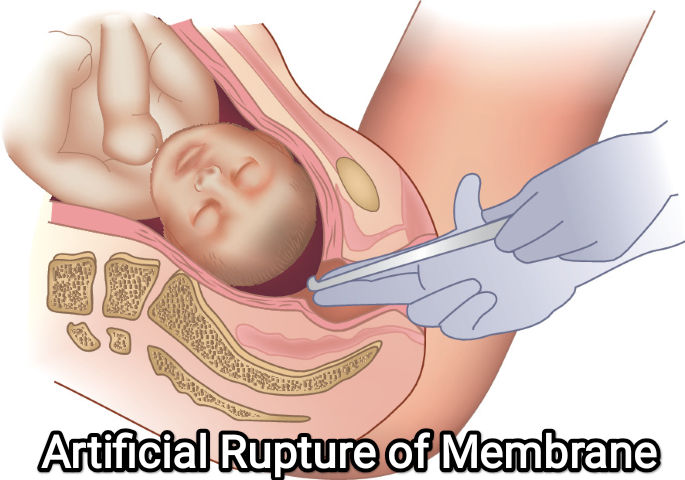
This will cause a gush or trickle of fluid to come out. The procedure may cause some discomfort but is usually not painful. The healthcare provider will then check the color, odor, and amount of the fluid, and monitor the baby’s heart rate and the mother’s contractions.
What are the benefits of Artificial Rupture of Membranes (AROM)?
AROM may have some benefits for labor progress and outcome, such as:
- Stimulating stronger and more regular contractions by releasing hormones and increasing pressure on the cervix.
- Shortening the duration of labor by an average of 40 to 90 minutes.
- Reducing the need for oxytocin (a synthetic hormone that induces contractions) or other interventions.
- Allowing for a more accurate assessment of the baby’s well-being by using an internal fetal monitor or checking the amniotic fluid for meconium (the baby’s first stool).
Indications for Artificial Rupture of Membranes:
- To augment or induce labor: AROM may be performed when labor progress is slow or needs to be induced. Breaking the amniotic sac can release prostaglandins and stimulate contractions, helping to speed up labor.
- Fetal monitoring: AROM can be done to facilitate continuous fetal monitoring, particularly when internal monitoring methods, such as a fetal scalp electrode, are required. This allows for a more accurate assessment of the baby’s well-being during labor.
- Meconium-stained amniotic fluid: If the amniotic fluid is stained with meconium (the baby’s first stool), AROM may be performed to assess the color and consistency of the meconium, which can provide information about fetal distress.
Contraindications for Artificial Rupture of Membranes:
- Abnormal fetal presentation: AROM is contraindicated if the baby’s presentation is abnormal, such as a transverse or breech position. In such cases, the rupture of membranes may cause umbilical cord prolapse, which is a dangerous situation.
- Unfavorable cervix: If the cervix is not yet dilated or if it is not effaced adequately, AROM may not be performed as it may increase the risk of complications, such as infection or prolonged labor.
- Suspected placental abruption: If there is a suspicion of placental abruption (premature separation of the placenta from the uterus), AROM is generally avoided, as it can exacerbate the condition and lead to further complications.
- Preterm labor: AROM is usually not performed if a woman is in preterm labor (before 37 weeks of gestation) unless there are specific medical reasons to do so. Premature rupture of membranes can increase the risk of infection and other complications in preterm infants.
It’s important to note that the decision to perform AROM is based on the healthcare provider’s assessment of the individual situation, weighing the potential benefits against the risks, and considering the woman’s overall health and medical history.
What are the risks of Artificial Rupture of Membranes (AROM)?
AROM also carries some risks and complications, such as:
- Increasing the risk of infection for both the mother and the baby, especially if labor is prolonged or if vaginal exams are frequent.
- Causing umbilical cord prolapse (when the cord slips out before the baby) or compression (when the cord is squeezed by the baby’s head), which can reduce blood flow and oxygen to the baby.
- Causing fetal distress or abnormal heart rate patterns due to changes in fluid pressure or temperature.
- Reducing the cushioning effect of the fluid, which may increase pain or discomfort for the mother or cause injury to the baby.
What are some alternatives to Artificial Rupture of Membranes (AROM)?
AROM is not always necessary or beneficial for labor. Some alternatives to AROM include:
- Waiting for spontaneous rupture of membranes (SROM), which usually happens naturally during labor or shortly before it begins.
- Using non-pharmacological methods to induce or augment labor, such as walking, nipple stimulation, acupressure, massage, or herbal remedies.
- Using pharmacological methods to induce or augment labor, such as oxytocin, prostaglandins, or misoprostol.
- Using external fetal monitoring or ultrasound to check the baby’s heart rate and amniotic fluid level.
What are some questions to ask your healthcare provider before the Artificial Rupture of Membranes (AROM)?
If your healthcare provider suggests AROM, you may want to ask some questions to make an informed decision, such as:
- Why do you recommend AROM to me?
- What are the benefits and risks of AROM for me and my baby?
- How will AROM affect my labor and delivery?
- How will you monitor me and my baby after AROM?
- What are some signs of infection or complications that I should watch out for?
- What are some alternatives to AROM that I can consider?
- How can I cope with pain or discomfort after AROM?
Nursing Responsibilities
The nursing responsibilities in artificial rupture of membrane (AROM):
Assess the patient’s condition.
This includes checking the patient’s vital signs, fetal heart rate, and uterine activity. The nurse should also assess the patient’s cervix to determine if it is effaced and dilated.
Explain the procedure to the patient and obtain consent.
The nurse should also answer any questions that the patient may have about the procedure.
Prepare the patient for the procedure.
This includes positioning the patient on her side, placing a towel under her buttocks, and providing privacy.
Assist the healthcare provider with the procedure.
The nurse may be asked to hold the patient’s legs, provide comfort measures, or monitor the fetal heart rate during the procedure.
Monitor the patient after the procedure.
This includes monitoring the patient’s vital signs, fetal heart rate, and uterine activity. The nurse should also assess the amount and color of amniotic fluid.
Document the procedure.
The nurse should document the time and date of the procedure, the amount and color of amniotic fluid, the fetal heart rate before and after the procedure, and any complications that occurred during or after the procedure.
Here are some additional nursing responsibilities that may be necessary depending on the patient’s condition:
- Administer pain medication as needed.
- Provide emotional support to the patient and her family.
- Educate the patient about what to expect after the procedure.
Nurses play an important role in the care of patients who have had AROM. By following the nursing responsibilities listed above, nurses can help to ensure that the patient has a safe and comfortable experience.
Conclusion
AROM is a common procedure that may be done during labor for various reasons. It may have some benefits for labor progress and outcome, but it also carries some risks and complications. It is important to discuss with your healthcare provider about the pros and cons of AROM and consider your preferences and options before agreeing to it. Remember that you have the right to accept or decline any intervention during your labor and delivery.
References
(1) Amniotomy – StatPearls – NCBI Bookshelf.
(2) Amniotomy (Breaking Your Water): How & Why It’s Done – Cleveland Clinic.
(3) Artificial rupture of membranes – Wikipedia.
(4) Artificial Rupture of the Membranes | SpringerLink.
FAQs
Q: What is the Artificial Rupture of Membranes (AROM)?
A: AROM stands for artificial rupture of membranes, which is a procedure in which the amniotic sac that surrounds the baby in the womb is intentionally ruptured by a healthcare provider.
Q: Why is Artificial Rupture of Membranes (AROM) done?
A: AROM may be done for various reasons during labor, such as to induce or speed up contractions, to monitor the baby’s heart rate more closely, or to check the amniotic fluid for signs of infection or fetal distress.
Q: How is AROM performed?
A: AROM is performed by inserting a gloved finger or a sterile instrument through the cervix and making a small tear in the membranes. This will cause a gush or trickle of fluid to come out.
Q: What are the benefits of AROM?
A: AROM may have some benefits for labor progress and outcome, such as stimulating stronger and more regular contractions, shortening the duration of labor, reducing the need for oxytocin or other interventions, and allowing for a more accurate assessment of the baby’s well-being.
Q: What are the risks of AROM?
A: AROM also carries some risks and complications, such as increasing the risk of infection for both the mother and the baby, causing umbilical cord prolapse or compression, causing fetal distress or abnormal heart rate patterns, and reducing the cushioning effect of the fluid.
Q: What are some alternatives to AROM?
A: Some alternatives to AROM include waiting for spontaneous rupture of membranes (SROM), using non-pharmacological or pharmacological methods to induce or augment labor, and using external fetal monitoring or ultrasound to check the baby’s heart rate and amniotic fluid level.
Q: What are some questions to ask your healthcare provider before AROM?
A: Some questions to ask your healthcare provider before AROM include why they recommend AROM for you, what are the benefits and risks of AROM for you and your baby, how will AROM affect your labor and delivery, how will they monitor you and your baby after AROM, what are some signs of infection or complications that you should watch out for, what are some alternatives to AROM that you can consider, and how can you cope with pain or discomfort after AROM.